
KEY TAKEAWAYS
- The ‘thunderclap headache’ — a severe headache reaching maximum intensity within 60 seconds — is a subarachnoid haemorrhage until proven otherwise and requires emergency evaluation.
- The phrase ‘worst headache of my life’ is not melodrama — it is a clinical red flag used by neurosurgeons globally to identify aneurysmal bleeds.
- Up to 40% of patients with a ruptured brain aneurysm experience a ‘sentinel headache’ — a sudden severe headache — days to weeks before the major rupture event.
- A normal CT brain in the emergency setting does not exclude subarachnoid haemorrhage — lumbar puncture or CT angiography is required if clinical suspicion remains.
- Unruptured aneurysms detected incidentally on MRI can often be managed electively with surgical clipping or endovascular coiling, with significantly better outcomes than emergency treatment after rupture.
- Dr. Sarang Gotecha performs cerebrovascular surgery including aneurysm clipping for patients across Pune and PCMC.
- Time from ictus to treatment is the single strongest predictor of outcome in ruptured aneurysm — minutes to hours matter.
Headache is the most common complaint in neurological practice. Tension headaches, migraines, cervicogenic headaches, dehydration headaches — almost everyone in Pune has experienced one. The vast majority are benign and self-limiting.
But a small fraction of headaches are not benign. They are the warning sign of a cerebrovascular catastrophe — a brain aneurysm leaking or rupturing. Distinguishing one from the other can be the difference between life and death, or between full recovery and permanent disability. This guide gives Pune patients and their families the tools to make that distinction and act accordingly.
QUICK FACTS
Thunderclap Headache Definition: Severe headache reaching maximum intensity within 60 seconds
SAH from Aneurysm — Mortality if Untreated: 50% within first month of rupture
Sentinel Headache Prevalence Before Major Rupture: Up to 40% of aneurysm patients
CT Sensitivity for SAH at 6 Hours: 98% — reduces to 85 to 90% after 24 hours
Unruptured Aneurysm Prevalence: ~3 to 5% of adults (most asymptomatic)
Time to Treatment Target: Within 24 to 48 hours of rupture for best outcomes
Headache Statistics and Aneurysm Data in India 2025-2026
| Metric | Data Point | Source |
| Prevalence of brain aneurysms in adults | 3 to 5% (most unruptured and asymptomatic) | Published literature |
| Annual SAH from aneurysm rupture in India | ~25,000 to 30,000 (Industry estimate) | Industry estimate |
| Mortality from ruptured aneurysm (untreated) | ~50% within 30 days | Published literature |
| Patients with sentinel headache before rupture | Up to 40% | Published literature |
| CT brain sensitivity for SAH at under 6 hours | ~98% | Published literature |
| Outcome with treatment within 24 hours vs delayed | Significantly better with early treatment | Published literature |
| Unruptured aneurysm annual rupture risk (under 7 mm) | ~0.5 to 1% per year | Published literature |
What Is a Brain Aneurysm?
A cerebral aneurysm is a balloon-like bulge in the wall of a brain artery, caused by a weakness in the arterial wall. Aneurysms most commonly form at arterial junctions — particularly in the circle of Willis at the base of the brain. They are present in approximately 3 to 5% of the adult population, most of which are small (under 7 mm), unruptured and entirely asymptomatic.
The danger is rupture. When an aneurysm ruptures, blood under high arterial pressure sprays into the subarachnoid space (the fluid-filled space between the brain and its coverings). This subarachnoid haemorrhage (SAH) causes sudden, extreme headache, neck stiffness, photophobia and frequently loss of consciousness. Without emergency treatment, 50% of patients die within 30 days of rupture. Of those who survive, many are left with permanent neurological deficits.
The Thunderclap Headache: How to Recognise It
The thunderclap headache is the clinical hallmark of subarachnoid haemorrhage. It is defined as a severe headache that reaches maximum intensity within 60 seconds of onset. Patients describe it as ‘like being hit on the back of the head with a cricket bat’, ‘an explosion inside my skull’ or simply ‘the worst headache I have ever had in my life’.
This is not typical headache language. Most tension or migraine headache patients describe a gradual build-up over minutes to hours. The thunderclap headache is instantaneous maximum pain. It is frequently accompanied by: brief loss of consciousness, neck stiffness (developing over hours), light sensitivity and nausea and vomiting. Any one of these features alongside a sudden maximum-intensity headache means call an ambulance, not wait and see.
The Sentinel Headache: The Warning Pune Patients Miss
Up to 40% of patients who have a major aneurysmal rupture describe a preceding period — days to weeks before the catastrophic event — of sudden severe headaches that resolved spontaneously. These are sentinel bleeds: small leaks from the aneurysm that cause pain but seal themselves. They are the body’s warning. Patients who present to a doctor after a sentinel headache and receive appropriate investigation can have their aneurysm treated before the major rupture.
Patients who attribute their sentinel headache to stress or a migraine variant and do not seek evaluation are denied this opportunity. In Pune, sentinel headaches are one of the most commonly missed clinical opportunities in cerebrovascular medicine. If you have experienced a sudden severe headache that was different from any headache you’ve had before — even if it resolved — a neurosurgical consultation with brain imaging is appropriate.
How to Distinguish a Dangerous Headache from a Benign One
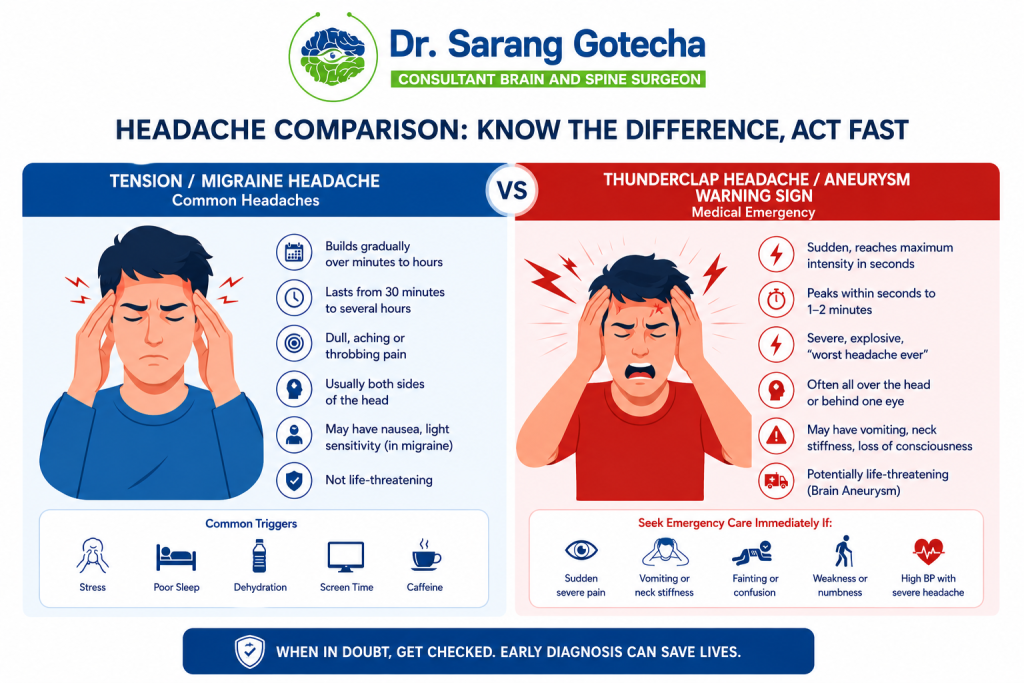
| Feature | Brain Tumor / Aneurysm Headache | Tension / Migraine Headache |
| Onset speed | Sudden — maximum within 60 seconds | Gradual — builds over 15 to 60 minutes |
| Severity | Worst of life | Moderate to severe, but familiar pattern |
| Time of day | Often during exertion or at rest | Often afternoon, evening, stress-related |
| Associated symptoms | Neck stiffness, photophobia, vomiting, LOC | Nausea, phonophobia, aura (migraine) |
| Previous history | New type of headache | Long-standing, recognisable pattern |
| Neurological signs | Possible weakness, speech change, vision loss | Aura — usually reversible |
| Response to painkillers | Variable — may not respond | Often responds to NSAIDs or triptans |
| Appropriate response | Emergency evaluation — same hour | GP or neurologist at next opportunity |
What Happens in Emergency: Investigation Pathway for SAH
If a patient with thunderclap headache arrives at a Pune emergency department, the first investigation is a non-contrast CT brain performed immediately. Within 6 hours of the bleed, CT detects subarachnoid blood in approximately 98% of cases — the blood appears bright white in the basal cisterns and sylvian fissures. After 24 hours, sensitivity drops to 85 to 90% as the blood becomes isodense with brain tissue.
If CT is positive, CT angiography (CTA) is performed immediately to identify the aneurysm location and morphology — information essential for planning surgical clipping or endovascular coiling. If CT is negative but clinical suspicion for SAH remains high, a lumbar puncture is performed to look for xanthochromia (yellow discolouration of CSF from blood breakdown products). A negative LP at 12 hours post-headache onset effectively excludes SAH.
Treatment Options for Brain Aneurysms in Pune
Surgical Clipping
Microsurgical clipping involves placing a small titanium clip across the neck of the aneurysm through a craniotomy, permanently excluding the aneurysm from the circulation. It is the more durable of the two treatment options — recurrence rates are under 2% at 10 years. For aneurysms in accessible locations with favourable morphology (wide neck, middle cerebral artery), clipping is often preferred.
Endovascular Coiling
Endovascular coiling is a catheter-based approach — a microcatheter is guided through the femoral artery to the brain aneurysm, and platinum coils are deployed to fill the aneurysm sac and induce clotting. No craniotomy is needed. Coiling is generally preferred for posterior circulation aneurysms and in elderly or medically fragile patients. Long-term recurrence rates are higher than clipping (10 to 20% require repeat treatment at 10 years).
The choice between clipping and coiling is made by the neurosurgeon and endovascular team together, based on aneurysm size, location, morphology and patient factors. Dr. Sarang Gotecha performs microsurgical aneurysm clipping as part of his cerebrovascular surgery practice in Pune.
Unruptured Aneurysm: Manage or Treat?
When a brain aneurysm is found incidentally — on an MRI done for another reason — the decision whether to treat it is nuanced. Small aneurysms (under 5 mm) in low-risk locations have an annual rupture risk of under 0.5% per year. For elderly patients with multiple comorbidities, surveillance (repeat MRI every 1 to 2 years) may be the most appropriate management. For younger, fit patients with larger aneurysms (over 7 mm) or aneurysms in higher-risk locations (posterior communicating, basilar tip), elective treatment before rupture significantly reduces lifetime rupture risk.
This decision should be made collaboratively between the patient and a neurosurgeon experienced in cerebrovascular surgery. The risks of elective treatment must be weighed against the risk of rupture — a calculation that requires knowledge of the patient’s specific aneurysm characteristics and overall health.
Cerebrovascular Emergency Care in Pune and PCMC
For patients in Pune, Baner, Wakad, Thergaon and PCMC who experience a thunderclap headache or witness a family member collapse with sudden severe headache: call for emergency transport to the nearest hospital with neurosurgical capability immediately. Do not drive yourself. Do not wait to see if it improves. Do not take pain medication and go to sleep.
Dr. Sarang Gotecha is available for cerebrovascular consultations including aneurysm clipping for patients across Pune and PCMC. For elective unruptured aneurysm consultations,
Frequently Asked Questions
Q: How do I know if my headache is a brain aneurysm?
The key distinguishing features of an aneurysm headache are: sudden onset reaching maximum severity within 60 seconds (thunderclap), described as the worst headache of your life, often accompanied by neck stiffness and light sensitivity, and frequently associated with brief loss of consciousness. If your headache fits this description, go to the emergency department immediately — do not wait for a GP appointment.
Q: What is a thunderclap headache?
A thunderclap headache is a severe headache that reaches its maximum intensity within 60 seconds of onset. It is the clinical hallmark of subarachnoid haemorrhage from a ruptured brain aneurysm. Not all thunderclap headaches are from aneurysms — other causes include reversible cerebral vasoconstriction syndrome and cerebral venous thrombosis — but every thunderclap headache requires emergency evaluation to exclude a life-threatening cause.
Q: Can a brain aneurysm cause headaches without rupturing?
Yes. Large unruptured aneurysms can cause headaches by compressing nearby brain structures or cranial nerves. A posterior communicating artery aneurysm can compress the third cranial nerve, causing a droopy eyelid and double vision alongside headache. A sudden severe headache without rupture — the sentinel headache — may indicate a small leak. Any new headache pattern in an adult should prompt neurological evaluation.
Q: What is the difference between surgical clipping and coiling for brain aneurysms?
Surgical clipping uses a small titanium clip placed around the aneurysm neck through a craniotomy — it is permanent with very low recurrence under 2%. Endovascular coiling fills the aneurysm sac with platinum coils through a catheter in the leg — no craniotomy needed, but higher recurrence rates of 10 to 20% over 10 years. The choice depends on aneurysm location, morphology and patient factors, determined by a neurovascular team.
Q: If my CT scan was normal after a severe headache, is it safe to go home?
Not necessarily. CT sensitivity for subarachnoid haemorrhage decreases after 24 hours — it is approximately 85 to 90% sensitive after that window. If clinical suspicion for SAH remains (thunderclap onset, neck stiffness, photophobia), a lumbar puncture at 12 hours post-headache is required to look for xanthochromia. A normal CT alone does not exclude SAH when the clinical story is suggestive.
Q: Does Dr. Sarang Gotecha perform brain aneurysm surgery in Pune?
Yes. Dr. Sarang Gotecha performs cerebrovascular surgery including microsurgical aneurysm clipping as part of his neurosurgical practice in Pune. He is available for consultations regarding both ruptured aneurysm management and elective unruptured aneurysm treatment decisions for patients from Pune, Baner, Wakad, Thergaon and PCMC. Book at drsaranggotecha.com.
Knowing the difference between a benign headache and a thunderclap headache could save your life or a family member’s life. The thunderclap headache — sudden, maximum intensity, worst ever, possibly with neck stiffness — is a neurosurgical emergency. The sentinel headache — a sudden severe headache that resolved — is a warning that deserves immediate investigation.
For cerebrovascular consultations, aneurysm management decisions and brain surgery expertise in Pune and PCMC, Dr. Sarang Gotecha is available at drsaranggotecha For acute emergencies, go directly to the nearest neurosurgical emergency department.

Dr. Sarang Gotecha
Dr. Sarang Gotecha is a leading brain & spine surgeon in Pune, offering advanced care for complex neurological and spinal conditions. With strong academic credentials (MBBS, MS, MCh Neurosurgery) and years of surgical experience, he is committed to delivering precise, safe, and patient-focused treatments.
- Expert in brain tumor, spine & neuroendoscopic surgeries
- Specialized in minimally invasive & skull base surgeries
- Follows an ethical and patient-centric approach
- Available at clinics in Baner, Wakad, and Thergaon (Pune)